


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jsurgery.bums.ac.ir/article-1-111-en.html


Adenoid nasopharyngeal ratio in children suffering from otitis media with effusion
Seyed Hasan Golboei1*, Gholamreza Sharifzadeh2, Sina Talebian3
1Assistant Professor, Department of Ear, Nose, and Throat Surgery, Faculty of Medicine, Birjand University of Medical Sciences, Birjand, Iran
2Assistant Professor, Social Determinants of Health Research Center, Birjand University of Medical Sciences, Birjand, Iran
3Student of Medicine, Faculty of Medicine, Birjand University of Medical Sciences, Birjand, Iran
Received: July 19, 2017 Revised: April 15, 2018 Accepted: May 16, 2018
|
Abstract Introduction: Otitis media (OM) is a major health problem that usually results from adenoid hypertrophy. The diagnosis is given based on symptoms and imaging studies, such as mouth breathing and lateral neck radiography (LNR), respectively. However, there are huge controversies regarding the LNR role in the management of patients with OM. This study aimed to evaluate adenoid nasopharyngeal ratio (AN ratio) in children suffering from OM with effusion (OME) and related factors. Methods: This cross-sectional study was conducted on 27OME-suspected children referring to the Ear, Nose and Throat clinics (ENT) affiliated with Mashhad University of Medical Sciences, Mashhad, Iran, in 2016. All the children underwent standard LNRs and indirect laryngoscopy in order to have adenoidal and nasopharyngeal length assessment before surgery. After adenoidectomy, pathologic data were analyzed in SPSS software (version 21) using Pearson correlation, independent sample t-test, and Mann-Whitney U test. P-value less than 0.05 was considered statistically significant. Results: According to the results, 70.4% of the participants were male. The mean age of the participants was 7.81±2.52 years. All the patients in the study were symptomatic, and the most frequent symptom was mouth breathing (100%). The mean values of AN ratio, pathologic adenoid size, and laryngoscopic adenoid size were 0.825±0.099, 18.22±5.97, and 5.33±19.15 mm, respectively. The AN ratio was significantly correlated with laryngoscopic and pathologic adenoid sizes (r=+0.46, P=0.01, and r=+0.44, P=0.02, respectively). Conclusions: The findings indicated a significant correlation between AN ratio and adenoid real measurement. Therefore, researchers are recommended to use this procedure in the assessment of patients with OME due to its availability, inexpensiveness, and negligible side effects. Key Words: Adenoidectomy, Laryngoscopy, Otitis media with effusion, Pathology, Physical examination, Radiography, Surgical |
Introduction
Otitis media (OM) is one of the most important public health problems, especially in the pediatric population of developing countries (1, 2). Untreated chronic serous OM is a serious threat to hearing ability, which has undergone a dramatic increase in recent years (3). The OM with effusion (OME) generally results from lymphoid tissue overgrowth in nasopharynx, chronic sinus infection, and allergies (4).
Nevertheless, inadequate treatment of acute
or subacute suppurative OM is an important contributor to the increased prevalence of chronic serous OM, causing mild and asymptomatic infection and thick mucoid effusion in the ear. Symptoms of OME are generally insignificant, including hearing loss with fluctuations during acute respiratory infections, feeling of heaviness or aural fullness, and impaired perception of sounds (5).
Otoscopy is the recommended primary examination for the diagnosis of OME; however, it may depict minor changes in the tympanic membrane and possibly a slight injury in tympanic membrane. Limited movement of the tympanic membrane in tympanometry and pneumatic otoscopy is the most useful otoscopic finding. The audiometric evaluation has a leading role in the diagnosis of conductive hearing loss. Long-term chronic serous OM may lead to the formation of cholesteatoma, tympanic membrane perforation, fibrosis in the middle ear, and tympanosclerosis, all of which may result in a permanent hearing loss. Therefore, the timely diagnosis and treatment of patients suffering from acute or chronic OME is crucial (6).
Adenoid hypertrophy is one of the underlying causes of OME resulting in a wide range of symptoms, such as runny nose, hyper nasality, OME, sleep disorders, and mouth breathing (7, 8). These symptoms indicate the association of adenoid hypertrophy with the obstruction of upper respiratory tract. Moreover, adenoid hypertrophy is one of the preliminary indications for adenoidectomy, which is one of the most common otorhinolaryngological surgeries (9). Surgical removal of a hypertrophic adenoid gland causes the disappearance of the respiratory symptoms and normal craniofacial development (10, 11).
Despite the numerous studies conducted on the diagnostic methods for the assessment of adenoid size, there is no standard and reliable technique for this purpose. Two of these methods are cavum X-ray and orthodontic cephalometric radiography, such as lateral neck radiography (LNR) (12, 13). Although these methods are inexpensive and available, they have a limited role in the assessment of animating areas, such as the ears (14).
Numerous ratios and criteria have been achieved based on the radiographic evaluation of this organ. Adenoid-nasopharyngeal ratio (AN ratio) is one of the most important and widely used criteria (12, 15-19), albeit there are several inconsistencies in the obtained results of various studies. In a study conducted by Wormald et al., no relationship was observed between AN ratio and size of adenoid in direct nasal endoscopy (17, 18). However, Cho et al. and Caylakli et al. showed a significant correlation between these two variables in 1999 and 2011, respectively (16, 19).
The findings of another study carried out by Kolo et al. in 2011, showed a direct association between the symptoms of children with airway obstruction and radiological findings (r=0.168, P=0.3); however, this relationship was insignificant (20). Lertsburapa et al. (2010) showed a positive correlation between adenoid gland measurement during surgery and AN ratio in LNR. Furthermore, they revealed that the estimation of adenoid
size by AN ratio resulted in a highly accurate measurement (21).
However, this method sometimes overestimates adenoid size when it is too small or too big (21). In a study conducted in India, AN ratio of ≥ 0.7 mm was reported as an adenoidectomy indicator
(22). Although in some studies, nasopharyngeal assessment has been accomplished by using LNR, AN ratio is inaccurate in the assessment of adenoid hypertrophy (12, 23). Therefore, the objective of this study was to evaluate AN ratio in children with OME and related factors.
Methods
This cross-sectional study was conducted on OME-suspected children referring to the Ear, Nose, and Throat clinics affiliated with Mashhad University of Medical Sciences, Mashhad, Iran, in 2016. The inclusion criteria were: 1) complaints about hearing loss, 2) conductive hearing loss of about 300 spin based on tuning fork test, 3) presence of diagnostic otoscopic criteria of OME (e.g., retraction of tympanic membrane, bulging tympanic membrane, membrane turbidity with reduced mobility with Valsalva maneuver, swollen malleus mostly with redness, and air-fluid levels), and 4) presence of tympanometry criteria of OME (i.e., type B tympanograms). On the other hand,
the exclusion criteria were: 1) unwillingness to participate, 2) history of otorhinolaryngological surgeries, and 3) congenital hearing loss.
Sample size was determined as 17 cases using a study conducted by Caylakli et al. (1) on the correlation of AN ratio and intraoperative findings of adenoid size (α=0.050 [type I error], β=0.200 [type II error], r=0.64). However, a total of 27 subjects were finally enrolled in the study .
C=0.5 * ln [(1+r)/(1-r)]=0.758
Total sample size: N=[(Zα+Zβ)/C] 2 + 3=17
The data were collected using a questionnaire covering information related to gender, age, and signs and symptoms of OME. A trained medical student gathered the information either via interviews with the children and their parents or by the examination of the patients' medical records. The content validity of the questionnaire was confirmed by five faculty members. Furthermore, adenoid and nasopharyngeal sizes, as well as nasopharyngeal adenoid ratio, were determined by radiography and physical examination.
All the included patients underwent LNR. To calculate the adenoidal size (line A), the distance between the outermost point of adenoid shadow and the line along sphenobasiocciput (line B) was measured. Moreover, the distance between the posterior edge of the hard palate and line B was estimated to obtain nasopharyngeal size (N).
Adenoid nasopharyngeal ratio was calculated through dividing adenoidal by nasopharyngeal size (Figure 1). All LNRs were reported by one radiologist using Fujioka method; in addition, to ensure the repeatability of the tools, all measurements were performed by the same person. Unit accuracy and measurement were reported in millimeters. After value extraction from the radiographs, they were multiplied by X-ray machine magnification (obtained from the radiologist) to calculate real values.
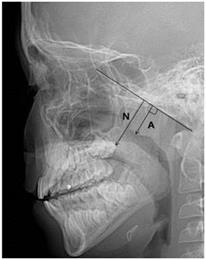
Figure 1: Estimation of the AN ratio (Fujioka Method).
The distance between the outermost point of convexity of adenoid shadow and sphenobasiocciput (A) is divided by the distance between sphenobasiocciput and the posterior end of the hard palate
Thereafter, the resulting numbers were used in the analysis. After initial diagnosis, the patients were examined in terms of laryngoscopic adenoid size by an otolaryngologist in the operating room prior to the surgery using indirect laryngoscopy (after anesthesia). Afterwards, the patients were subjected to adenoidectomy, and the tissues were sent to the pathology laboratory for pathologic evaluation. All samples were reviewed and approved by a pathologist.
Ethical consideration
Research approval was obtained from the Ethics Committee affiliated with the Medical School of Birjand University of Medical Sciences, Birjand, Iran. Written informed consent was attained from the legal guardians of children in order to include them in the study. Data were collected without name, and confidentiality of the data was maintained. Moreover, informed consent was obtained from all patients, and the ethical protocol of the design (Identifier: Ir.bums.REC.1395.166) was approved by the Ethics Committee of Birjand University of Medical Sciences, Birjand, Iran.
Statistical analysis
The data were analyzed in SPSS (version 21) and were described using frequency tables, graphs, mean indices, and standard deviation. Before analysis, the normality of the data was analyzed using the Kolmogorov-Smirnov test, indicating that radiologic adenoid size and AN ratio had normal distribution (P=0.13 and P=0.14, respectively).
On the other hand, radiologic nasopharyngeal size had a non-symmetric distribution (P=0.03). Pearson's correlation coefficient was used to determine the relationship between the AN ratio and adenoidal size. To compare mean AN ratio and radiologic adenoid size, independent t-test was employed. Moreover, due to the non-normal distribution, U Mann-Whitney test was utilized for the quantitative variables to compare the average size of radiologic nasopharyngeal. P-value less than 0.05 was considered statistically significant.
Results
A total of 27 children, including 19 males (70.4%) and 8 females (29.6%), with a mean age of 7.81±2.52 years participated in the study. The majority of the patients were at least 8 years old (n=14, 51.9%) (Table 1). All patients in this study were symptomatic (n=27, 100%) and the most common symptoms were reported as mouth breathing, snoring, and hyponasal speech as reported in 27, 25, and 8 cases, respectively.
The mean values of pathologic adenoid size, laryngoscopic adenoid size, and radiologic AN ratio were obtained as18.69±3.29 (range: 12.5-30),
Table 1: Demographic distribution characteristics of the study
|
|
|
Frequency |
Percentage |
|
Gender |
Male Female |
19 8 |
70.4 29.6 |
|
Age |
Below 7 years Above 8 years |
13 14 |
48.1 51.9 |
22.75±3.62 (range: 17-33), and 0.825±0.099 mm (range: 0.54-1), respectively. Furthermore, the pathologic and endoscopic adenoid sizes were reported as 18.22±5.97 (range: 10-25) and 19.15±5.33 mm (range: 10-30), respectively.
There was no direct relationship between the mean AN ratio and age among the children with OME (t=0.072, P=0.9). The mean adenoid sizes in patients younger than seven and older than eight years were 18.72±4.46 and 18.66±1.84 mm (t=0.045, P=0.9), respectively. The results revealed no significant difference between these groups in terms of mean nasopharyngeal size (P=0.6). In addition, adenoid size on LNR was higher in males than in females (19.41±3.27 vs. 16.97±2.84 mm, P=0.08). Furthermore, there was no significant difference between the male and female patients in terms of nasopharyngeal size and AN ratio (P>0.05).
Moreover, the results showed no significant difference among AN ratio and pathologic adenoid size, and nasopharyngeal size with respect to different symptoms (tables 2 and 3). However, a positive correlation was obtained between AN ratio and endoscopic and pathologic adenoid size (r=+0.46, P=0.01, r=+0.44, P=0.02, respectively).
Table 2: The Comparison of average adenoidal-nasopharyngeal ratio (A/N ratio), adenoid size, and nasopharyngeal size in children suffering from otitis media with effusion according to age and gender
|
|
AN ratio (mm) X̅± SD |
Independent t test |
|
|
Age |
7 years or less 8 years and more |
0.827±0.106 0.824±0.097 |
t=0.072 p=0.9 |
|
Gender |
Male Female |
0.829±0.081 0.816±0.141 |
t=0.319 p=0.75 |
|
|
adenoid size mean (mm) X̅± SD |
||
|
Age |
7 years or less 8 years and more |
18.72±4.46 18.66±1.84 |
t=0.045 p=0.9 |
|
Gender |
Male Female |
19.41±3.27 16.97±2.84 |
t=1.83 p=0.08 |
|
|
Nasopharyngeal size mean (mm) |
U Mann-Whitney test |
|
|
Age |
7 years or less 8 years and more |
13.15 14.79 |
z=-0.536 p=0.6 |
|
Gender |
Male Female |
15.53 10.38 |
z=-1.547 p=0.1 |
Table 3: The comparison of average adenoidal-nasopharyngeal ratio (A/N ratio), adenoid size, and nasopharyngeal size in children suffering from otitis media with effusion (OME) according to different symptoms
|
|
Snoring |
Independent t test |
|
|
Yes (X̅±SD) |
No (X̅±SD) |
||
|
Adenoidal-nasopharyngeal ratio |
0.82±0.1 |
0.84±0.02 |
t=-0.5 p=0.6 |
|
Adenoid size |
18.78±3.41 |
17.55±0.91 |
t=0.3 p=0.7 |
|
Nasopharyngeal size |
Yes (mean rank) |
No ( mean rank) |
U Mann-Whitney test |
|
14.4 |
9 |
z=-0.9 p=0.3 |
|
|
|
Hyponasal speech |
Independent t test |
|
|
Yes (X̅±SD) |
No (X̅±SD) |
||
|
Adenoidal-nasopharyngeal ratio |
0.78±0.06 |
0.80±0.10 |
t=1.65 p=0.1 |
|
Adenoid size |
19.46±3.41 |
18.36±2.66 |
t=0.78 p=0.4 |
|
Nasopharyngeal size |
Yes (mean rank) |
No ( mean rank) |
|
|
11.75 |
14.95 |
z=0.9 p=0.3 |
|
Discussion
The results of this study indicated no correlation between ratio LNR and nasopharyngeal size, AN ratio, and other variables such as different symptoms, gender, and age. In a study conducted by Caylakli et al. on the relationship between
AN ratio and adenoid hypertrophy, a positive correlation was reported based on endoscopic examination findings (P<0.0001). The results of the mentioned study are consistent with our findings on the correlation between AN ratio and adenoid gland measurement during surgery and pathological examination (19).
In line with our data, Letsburapa et al. demonstrated an association between adenoid size in nasal endoscopy and radiographic measurements. They concluded that LNR could accurately estimate adenoid size (21). However, it should be considered that LNR measurements overestimate adenoid size if the actual size of adenoid is too small. Furthermore, adenoid size could be underestimated in LNR assessment if the actual adenoid size is too big (21).
The results of several studies are inconsistent with those of the current study (12, 23). In this regard, Mlynarek et al. comparing the radiologic adenoid size using LNR and direct video rhinoscopy revealed that the increase in AN ratio was not consistent with adenoid enlargement in video rhinoscopy (P=0.082, r=0.312) (12). In a study performed by Al-Kindy et al. on the significance of radiological findings in the treatment of children with adenoidal hypertrophy, about 30% of symptomatic children underwent adenoidectomy (23). They concluded that more than 70% of the patients were treated medically and that radiological findings had a limited role in the management of adenoidal hypertrophy. Therefore, they did not recommended to routinely use radiological procedure for a therapeutic purpose (23).
In the mentioned study, the lateral neck radiographs of patients showed increased adenoid size resulting from acute inflammation; however, this acute adenoid inflammation improved after medical treatment and removed the need for adenoidectomy. As a results, there was no correlation between the patients’ symptoms and adenoid nasopharyngeal ratio (23). Likewise, in a study examining the radiographic evaluation of children with obstructive adenoid, Kolo et al. reported a weak and insignificant correlation between symptom presence and radiological findings (r=0.168 and P=0.3) (20).
In another study, Mlynarek et al., compared lateral neck radiography and direct video rhinoscopy in adenoid measurement and observed no correlation between adenoid nasopharyngeal ratio and symptom presence (rho=-0.073, P=0.69) (12). Inconsistent with this study, Gangadhara
et al., evaluating the significance of adenoid nasopharyngeal ratio in the assessment of adenoid hypertrophy in children, reported that the patients who presented with mouth breathing and snoring symptoms had a significantly larger adenoid (24).
Conclusions
The results of the present study showed that AN ratio had a significant correlation with adenoid real measurement (in pathology and during surgery). The LNR is inexpensive and accessible and has negligible side-effects, which can be used in the management of adenoid hypertrophy. Further studies are recommended to investigate the children with adenoid hypertrophy symptoms whose adenoid enlargement is confirmed using LNR and AN ratio and who have undergone medical treatment before adenoidectomy. Then, radiological examination needs to be repeated on the patients and adenoid and pharyngeal size and their ratio and changes should be assessed. At the end, the correlation of AN ratio changes and adenoidectomy is required.
Acknowledgments
Authors gratefully acknowledge Dr. Jafarian for his kind help in reporting the pathologic findings of tissues. We also acknowledge the great support of Dr. Abbasi in the interpretation of the radiologic studies.
Author’s contribution
Seyed Hasan Golbuihe suggested the main idea of the study and contributed to the writing of the manuscript. Gholamreza Sharifzadeh performed the data analysis. Sina Talebian performed data collection and involved in writing the manuscript.
Funding
No funding is received from a known source.
Conflict of Interest
There are no conflicts of interest to declare.
References
1. Mahadevan M, Navarro-Locsin G, Tan HK, Yamanaka N, Sonsuwan N, Wang PC, et al. A review of the burden of disease due to otitis media in the Asia-Pacific. Int J Pediatr Otorhinolaryngol. 2012; 76(5):623-35. DOI: 10.1016/j.ijporl.2012.02.031P
2. Prakash R, Juyal D, Negi V, Pal S, Adekhandi S, Sharma M, et al. Microbiology of chronic suppurative otitis media in a tertiary care setup of uttarakhand state, India. N Am J Med Sci. 2013; 5(4):282-7. DOI: 10.4103/1947-2714.110436P
3. Wu JF, Jin Z, Yang JM, Liu YH, Duan ML. Extracranial and intracranial complications of otitis media:
22-year clinical experience and analysis. Acta Otolaryngol. 2012; 132(3):261-5. DOI: 10.3109/
00016489.2011.643239P
4. Farajzadah Sheikh A, Saki N, Roointan M, Ranjbar R, Yadyad MJ, Kaydani A, et al. Identification of alloiococcus otitidis, streptococcus pneumoniae, moraxella catarrhalis and haemophilus influenzae in children with otitis media with effusion. Jundishapur J Microbiol. 2015; 8(3):e17985. DOI: 10.5812/jjm.
17985P. PMC4386075
5. Kong K, Coates HL. Natural history, definitions, risk factors and burden of otitis media. Med J Aust. 2009; 191(9 Suppl):S39-43.
6. Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, et al. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ. 2010; 340:c1594. DOI: 10.1136/bmj.c1594P. PMC2857748
7. Dolen WK, Spofford B, Selner JC. The hidden tonsils of Waldeyer's ring. Ann Allergy. 1990; 65(4):244-8.
8. Wang DY, Bernheim N, Kaufman L, Clement P. Assessment of adenoid size in children by fibreoptic examination. Clin Otolaryngol Allied Sci. 1997; 22(2):172-7.
9. T-Ping C, Weckx LL. ENT care of children and adolescents in the Brazilian public healthy system in three different municipalities. Braz J Otorhinolaryngol. 2008; 74(4):571-8.
10. Brietzke SE, Brigger MT. Adenoidectomy outcomes in pediatric rhinosinusitis: a meta-analysis. Int J Pediatr Otorhinolaryngol. 2008; 72(10):1541-5. DOI: 10.1016/
j.ijporl.2008.07.008P
11. Peltomäki T. The effect of mode of breathing on craniofacial growth--revisited. Eur J Orthod. 2007; 29(5):426-9. DOI: 10.1093/ejo/cjm055P
12. Mlynarek A, Tewfik MA, Hagr A, Manoukian JJ, Schloss MD, Tewfik TL, et al. Lateral neck radiography versus direct video rhinoscopy in assessing adenoid size. J Otolaryngol. 2004; 33(6):360-5.
13. Kemaloglu YK, Goksu N, Inal E, Akyildiz N. Radiographic evaluation of children with nasopharyngeal obstruction due to the adenoid. Ann Otol Rhinol Laryngol. 1999; 108(1):67-72.
14. Aboudara CA, Hatcher D, Nielsen IL, Miller A. A three-dimensional evaluation of the upper airway in adolescents. Orthod Craniofac Res. 2003; 6(Suppl 1):173-5.
15. Fujioka M, Young LW, Girdany BR. Radiographic evaluation of adenoidal size in children: adenoidal-nasopharyngeal ratio. AJR Am J Roentgenol. 1979; 133(3):401-4. DOI: 10.2214/ajr.133.3.401P
16. Cho JH, Lee DH, Lee NS, Won YS, Yoon HR, Suh BD. Size assessment of adenoid and nasopharyngeal airway by acoustic rhinometry in children. J Laryngol Otol. 1999; 113(10):899-905.
17. Wormald PJ, Prescott CA. Adenoids: comparison of radiological assessment methods with clinical
and endoscopic findings. J Laryngol Otol. 1992; 106(4):342-4.
18. Chami FA. Avaliaçäo nasofibroscópica e rediológica de pacientes com hiperplasia da amígdla faríngea. Rev Bras Med Otorrinolaringol. 1998; 5(4):118-28.
19. Caylakli F, Hizal E, Yilmaz I, Yilmazer C. Correlation between adenoid-nasopharynx ratio and endoscopic examination of adenoid hypertrophy: a blind, prospective clinical study. Int J Pediatr Otorhino-laryngol. 2009; 73(11):1532-5. DOI: 10.1016/j.ijporl.
2009.07.018P
20. Kolo ES, Ahmed AO, Kazeem MJ, Nwaorgu OG. Plain radiographic evaluation of children with obstructive adenoids. Eur J Radiol. 2011; 79(2):e38-41. DOI: 10.1016/j.ejrad.2010.09.027P
21. Lertsburapa K, Schroeder JW Jr, Sullivan C. Assessment of adenoid size: a comparison of lateral radiographic measurements, radiologist assessment, and nasal endoscopy. Int J Pediatr Otorhinolaryngol. 2010; 74(11):1281-5. DOI: 10.1016/j.ijporl.2010.08.005P
22. Sharifkashani S, Dabirmoghaddam P, Kheirkhah M, Hosseinzadehnik R. A new clinical scoring system
for adenoid hypertrophy in children. Iran J Otorhinolaryngol. 2015; 27(78):55-61.
23. Al-Kindy SA, Obaideen AO. The value of radiological examination in the management of adenoidal hypertrophy in a pediatric population. Saudi Med J. 2003; 24(5):504-6.
24. Gangadhara KS, Rajeshwari A, Jain M. Significance of adenoid nasopharyngeal ratio in the assessment of adenoid hypertrophy in children. Res Otolaryngol. 2012; 1(1):1-5. DOI: 10.5923/j.otolaryn.20120101.01
Received: 2017/07/19 | Accepted: 2018/05/16 | Published: 2018/11/14 | ePublished: 2018/11/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Attribution-NoneCommercial CC BY-NC
