



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jsurgery.bums.ac.ir/article-1-211-en.html


Trauma-related amputations among children in Ghana
Alexis Buunaaim D.B1![]() , Waliu Jawula Salisu2
, Waliu Jawula Salisu2![]() , Yempabe Tolgou3*
, Yempabe Tolgou3*![]() , Hamdiyat Abdulai S.4
, Hamdiyat Abdulai S.4![]()
1MD, Department of Surgery, School of Medicine and Health Sciences, University for Development Studies, Tamale, Ghana
2Ph.D. Candidate, Department of Nursing, Tamale Teaching Hospital, Tamale, Ghana
3MD, Department of Surgery, Trauma and Orthopedics Unit, Tamale Teaching Hospital, Tamale, Ghana
4BSc, Department of Research and Development, Tamale Teaching Hospital, Ghana
Received: October 01, 2019 Revised: December 17, 2019 Accepted: January 11, 2020
|
Abstract Introduction: Amputation operations are rare in children and are often performed in emergencies as lifesaving procedures or in elective cases resulting from congenital limb deficiencies. This study aimed to retrospectively examine the pattern of trauma-related amputations among children in Ghana. Methods: Hospital records of the children aged 16 years and younger who underwent trauma-related amputations during May 2015-September 2018 were assessed retrospectively. The data were analyzed using the SPSS software version 24 (IBM, Chicago, USA). Descriptive statistics were used to report the means and frequencies. Results: A total of 34 children had amputation surgeries during the study period. Our findings showed that 5.9% (n=2) of the subjects were female and 94.1% (n=32) were male. Falls as the leading cause accounted for 50% (n=17) of the injuries, followed by personal or interpersonal violence 23.5% (n=8), road traffic accidents 14.7% (n=5), machinery 5.9% (n=2), and birth injuries mainly related to the accidents during child delivery 5.9% (n=2). At the onset of injury, 61.8% (n=21) of the children were taken to hospitals as the first point of call, while 38.2% of the cases (n=13) first referred to bonesetters. According to the records, upper limb amputation 70.6% (n=24) was more frequent than lower limb 29.4% (n=10). Conclusions: A record of thirty-four trauma-related amputations among children over a period of 3.5 years in a single treatment center is remarkable. The living environment of children could predispose them to catastrophic incidents leading to amputations. Therefore, strategies for injury prevention should be developed taking into consideration the contextual factors. Key words: Adult children, Amputation, Child, Multiple trauma |
Introduction
Amputation operations are rare in children and are often carried out in emergencies as lifesaving procedures (1, 2) or as planned cases resulting from congenital limb deficiencies (3). Regardless of the case and reason, losing a limb is a difficult and emotional situation for the patient, family, and health professionals who are directly involved in the care of the patient.
Trauma-related amputations are the most typical form of acquired amputations among children (4). Although there are variations based on geographical locations, most studies suggest the most frequent causes of childhood traumatic amputations as power tools, road traffic accidents, machinery, and gun-related wounds (3-5). Male children are more frequently reported as the victims, compared to their female counterparts
(2, 6-8).
Traumatic amputations pose dire consequences to both patients and their caregivers, often requiring expensive surgical procedures, rehabilitation, and expertise (9). In addition, the literature suggests that osseous overgrowths may develop later in life requiring further surgical procedures (9, 10) that result in the possibility of further financial and psychological burden on caregivers.
Trauma-related amputations are often performed in haste to save the life of the child. Nonetheless, the orthopedic surgeon must pay critical attention to the basic principles of creating a prosthesis-friendly stump (1) as this will be necessary for future decisions regarding prosthetic fittings. Limb prosthesis provides physical support for children and enables them to participate in some activities of daily living (8, 11). Moreover,
the prosthesis is considered as a mean for psychological adjustment to limb loss.
However, in most developing countries, access to prosthesis and rehabilitation is limited (12). A situation that leaves most amputee children in a stressful state as they often find it challenging to cope with the physical needs of the body. As a result, they are withdrawn from critical social activities, such as school and sports activities, which leads to lifelong depression.
In Ghana and most of the sub-Saharan Africa region, the epidemiology of trauma-related amputations in children or the availability of post-amputation support for this vulnerable group is not well documented. Therefore, the aim of this study was to examine the pattern of trauma-related amputations in children.
Methods
The current study is a part of a more extensive review of amputations in a major referral hospital. This retrospective descriptive study was carried out at Tamale Teaching Hospital (TTH), which is a major referral center in northern Ghana. This teaching hospital is affiliated to the School of Medicine and Health Sciences, University for Development Studies. Being the biggest referral hospital in the entire northern part of Ghana, it is currently an 800-bed facility with various specialties, including a Trauma and Orthopedics Unit.
The records of children aged 16 years and younger who underwent a trauma-related amputation during May 2015-September 2018 in the Trauma and Orthopedics Unit of Tamale Teaching Hospital were examined in this study. The cases with non-traumatic amputation were excluded from the investigation.
The demographic data and clinical history of the participants were recorded and analyzed in this study. This information included the mechanism of injury, site of the fracture, site of amputation, the first point of call, reasons for referring to the hospital in case the first point of call was not a hospital, and time of presentation to hospital after injury. The data were analyzed using the SPSS software version 24 (IBM, Chicago, USA). Descriptive statistics were used to report the means and frequencies.
It should be noted that no patients were involved in this study due to the retrospective design for evaluating the data of patients. However, we obtained ethical approval for the current study from the Ethics Committee of Tamale Teaching Hospital with the code of TTHERC/17/11/16/04.
Results
A total of 34 children aged between 7 days to 16 years had amputation surgeries during the study period. The results indicated that male children with the frequency of 94.1% (n=32) outnumbered females with the frequency of 5.9% (n=2) by a ratio of 16:1. The mean age of the study participants was 9.5±4.63 years.
According to our evaluations, the mechanisms of injury could be categorized into five broader headings, namely falls, personal and interpersonal violence, road traffic accidents, machinery, and birth injuries, which accounted for 50% (n=17), 23% (n=8), 14.7% (n=5), 5.9% (n=2), and 5.9% (n=2) of the total cases, respectively. We believe that these results can serve as a basis for easy comparison with the findings of previous studies. Detailed age distribution and other demographics are presented in Table 1.
Regarding the site of amputation, 38.2% (n=13), 32.4% (n=11), 17.6% (n=6), and 11.8% (n=4) of the cases were below elbow (BEA), above elbow (AEA), below knee, and above knee amputations, respectively. In general, upper limb loss 70.6% (n=24) was reported to be more frequent than lower limb loss 29.4% (n=10).
According to our results, 61.8% (n=21) of the children were taken to the hospital as the first point of call after the injury, while 38.2% (n=13) were reported to first refer to bonesetters. As
Table 1: Demographic characteristics of the participants
|
|
Frequency (n) |
Percentage |
|
|
Gender |
Male |
32 |
94.1 |
|
Female |
2 |
5.9 |
|
|
Age |
5 years and younger |
10 |
29.4 |
|
6-10 years |
8 |
23.5 |
|
|
11-16 years |
16 |
47.1 |
|
|
Time of presentation |
≤5 h |
14 |
41.2 |
|
6-24 h |
7 |
20.6 |
|
|
25-72 h |
2 |
5.9 |
|
|
≥73 h |
11 |
32.4 |
|
|
Mechanism of injury |
Machinery |
2 |
5.9 |
|
Road traffic accidents |
5 |
14.7 |
|
|
Falls |
17 |
50 |
|
|
Personal or interpersonal violence |
8 |
23.5 |
|
|
Birth injury |
2 |
5.9 |
|
|
Site of fracture |
Upper limb |
24 |
70.6 |
|
Lower limb |
10 |
29.4 |
|
|
Site of amputation |
Above elbow |
11 |
32.4 |
|
Below elbow |
13 |
38.2 |
|
|
Below knee |
6 |
17.6 |
|
|
Above knee |
4 |
11.8 |
|
shown in Table 1, we categorized the subjects based on the time of presentation after injury occurrence into the groups of ≤ 5, 6-24, 25-72, and ≥ 73 h with the frequencies of 41.2% (n=14), 20.6% (n=7), 5.9% (n=2), and 32.4% (n=11), respectively.
Furthermore, the reasons for the referral of the patients to the hospital were assessed in case the first point of call was not a hospital. It was revealed that 13 participants (38.2%) belonged to this category that first referred to traditional bonesetters before referring to a hospital due to complications. Overall, 76.9% (n=10) of the patients referred to the hospital with gangrene (Figure 1), 15.4% (n=2) with infections, and 7.7% (n=1) with massive swellings associated with pain (Figure 2). In addition, the mean length of stay was recorded as 23±20.7 days.
Discussion
To our knowledge, this is the first study in sub-Saharan Africa that focuses on trauma-related amputations among children. Consequently, this research will likely be a yardstick for future studies in this area.
Although the reports of post-amputation deaths are remarkable among adult age groups (13), no case of death was recorded in the current study. Among the 34 participants of the present study, male children dominated their female counterparts by a wide margin. This is consistent with the findings of similar studies that observed a higher incidence in male subjects than females in the United Kingdom (6) and the United States of America (USA) (9).
Contrary to the investigation performed by Roche and Selvarajah (6), a higher rate of upper limb (70.6%) loss was found, compared to the lower limb (29.4%). However, these findings are consistent with similar studies conducted in the USA (9) and Pakistan (8). We believe that this controversy could be attributed to environmental and geographical factors. Most children tend to explore their immediate environment using the upper limbs, which more predisposes them to the traumatic injuries of the upper section of the body than the lower. As a result, we believe that children who live in areas where they are exposed to potentially dangerous objects would be more likely to acquire upper limb injuries.
Moreover, we found falls as the most common cause of amputation among the study participants (50%), followed by interpersonal violence (23.5%) and road traffic accidents (14.7%). However, this is not in line with the results of the previous studies that reported power tools (4), vehicular accidents (6), and burns (8, 14) as the primary causes of trauma among children. Our findings suggest that environmental factors play a role in these incidents

1 Nine-year-old boy brought to the hospital with gangrene following a previous local treatment of the fracture by a traditional bonesetter
Figure 1: Limb gangrene
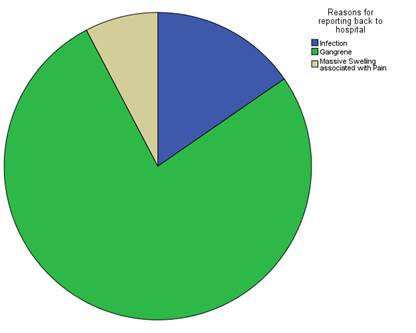
2 Reasons for referral to the hospital after being taken to traditional bonesetters
Figure 2. Reasons for referral to hospital
that lead to amputations. The influential factors tend to vary based on the geographical location of children, such as urban, peri-urban, and rural areas, as well as developing, middle income, and developed countries.
An essential aspect of the costs in the treatment procedure of trauma-related amputations is associated with the length of hospital stay. The need for revising surgeries, management of infections, and rehabilitation could warrant more extended hospital stays. Based on our findings, the maximum and minimum days spent in the hospital were 82 and 2 days, respectively. The cost of amputation surgery regardless of the expenses of medications, anesthesia, and prosthesis in this study setting was US$ 67.5, while US$ 4.9 was required for each day spent on admission. Therefore, more extended hospitalization is cost-intensive to the patient and family.
Approximately 38.2% of the study population first referred to bonesetters before a hospital. A majority of this subgroup of participants reported with gangrene, followed by infections, and
other complications. These sequels contribute significantly to the prolongation of hospital stays resulting in the increased financial and psychological burden of caregivers. It is noteworthy that 76% of patients with long hospital stays were either those who referred to the hospital after bonesetters or referred late after the onset of the injury.
In most of the developing countries, including Ghana, bonesetters play an essential role in managing fractures using traditional and unscientific methods. However, their activities mostly account for severe complications resulting in amputation and other health risks, especially among children (15).
For example, most children among the subjects of this study referred to the hospital complaining from complications due to referral to bonesetters for supracondylar fractures. One of the most frequent complications of supracondylar fracture is compartment syndrome caused by massive swelling. However, the bonesetters usually cover the fracture sites with black substances believed to be medicinal, tie with the strands of tiny sticks, and leave it in place for several days, hoping the fracture would resolve.
These innocent children go through anguishing pain for several days as the site gets inflamed with the surrounding tissues gradually developing necrosis. Nonetheless, the bonesetter is usually still hopeful that the child will be healed until the complications become unbearable and noticeable and they consider referral to hospitals.
Several studies have reported the role bonesetters play in the mismanaging and complicating of fractures (16-18). Subsequently, it is not surprising that some authors are attempting to make the activities of bonesetters regulated (19). With this background in mind, we recommend extensive public education in this regard.
After successfully undergoing amputations, amputee children face numerous physical and psychosocial challenges with possible denting implications in future functionality and ambitions. As a result, rehabilitation and obtaining the right prosthesis are crucial in providing some psychological and physical support. However, we observed that a considerable number of the parents of amputee children in this region feel reluctant to discuss the possibility of rehabilitation and the acquisition of prosthesis.
Ahmad et al. in a different setting suggested the latter issue to be partly due to the economic reasons (5) and the fact that these services are rarely available or mostly nonfunctional (20) in this part of the world. Currently, there are no prosthetic services in the entire northern part of Ghana. Few patients who can afford these services have to travel far down South to Nsawam, a town near Accra, which houses the only functional lower limb prosthesis service center in the entire country.
Conclusions
The record of 34 trauma-related amputation cases among children in a single treatment center during a period of 3.5 years is a remarkable number. In the current study, upper limb amputations were the most frequent pattern. Furthermore, we found that falls, interpersonal violence, and road traffic accidents were the common mechanisms of injury resulting in amputations at the site of this investigation.
According to the literature, the immediate living environment of children could predispose them to such catastrophic incidents. Therefore, strategies should be developed to prevent injuries, especially for falls as the leading cause of such amputations. Other contextual factors should be taken into consideration in such attempts. Amputee children benefit from rehabilitation and prosthesis as a source of psychological and physical support. Consequently, we recommend that major referral hospitals and trauma management centers be well equipped to provide these services at affordable costs.
Acknowledgments
The authors of this study would like to thank the staff of the Trauma and Orthopedics Unit and Registry Department of Tamale Teaching Hospital for their cooperation during the phase of data gathering for the current investigation.
Funding
The authors did not receive any financial support for the present study.
Conflict of Interest
There is no conflict of interests to be declared.
References
1. Griffet J. Amputation and prosthesis fitting in paediatric patients. Orthop Traumatol Surg Res. 2016; 102(1):S161-75. PMID: 26797004 DOI: 10.1016/j.otsr.2015.03.020
2. de Godoy JM, de Godoy LM. Epidemiological data of amputations in children. Clin Pediatr Dermatol. 2016; 2:1-3. Doi: 10.21767/2472-0143.100016
3. Smith DG. Congenital limb deficiencies and acquired amputations in childhood, part 3. Motion. 2006; 16(1):41-5.
4. Tooms RE. Acquired amputations in children. Digital Resourse Found. 2002; 32:2-8.
5. Ahmad J, Gupta AK, Sharma VP, Kumar D, Yadav G, Singh S. Traumatic amputations in children and adolescents: A demographic study from a tertiary care center in Northern India. J Pediatr Rehabil
Med. 2016; 9(4):265-9. PMID: 27935565 DOI: 10.3233/PRM-160398
6. Roche AJ, Selvarajah K. Traumatic amputations in children and adolescents. J Bone Joint Surg Br. 2011; 93-B(4):507-9. PMID: 21464491 DOI: 10.1302/0301-620X.93B4.25719
7. Ogeng'o JA, Obimbo MM, King'ori J. Pattern of limb amputation in a Kenyan rural hospital. Int Orthop. 2009; 33(5):1449-53. PMID: 19475408 DOI: 10.1007/s00264-009-0810-5
8. Sami AL, Anjum N, Shaukat M, Hanif A, Siddique K. Pattern and mode of trauma for child amputation at tertiary care hospital. Ann King Edward Med Univ. 2012; 18(1):81. DOI: 10.21649/akemu.v18i1.380
9. Conner KA, McKenzie LB, Xiang H, Smith GA. Pediatric traumatic amputations and hospital resource utilization in the United States, 2003. J Trauma. 2010; 68(1):131-7.
10. Vocke AK, Schmid A. Osseous overgrowth after post-traumatic amputation of the lower extremity in childhood. Arch Orthop Trauma Surg. 2000; 120(7-8):452-4. PMID: 10968538 DOI: 10.1007/s0040
29900128
11. Rajťúková V, Michalíková M, Bednarčíková L, Balogová A, Živčák J. Biomechanics of lower limb prostheses. Proc Eng. 2014; 96:382-91. DOI: 10.1016/j.proeng.2014.12.107
12. Yinusa W, Ugbeye ME. Problems of amputation surgery in a developing country. Int Orthop. 2003; 27(2):121-4. PMID: 12700939 DOI: 10.1007/
s00264-002-0421-x
13. de Godoy JM, Ribeiro JV, Caracanhas LA. Hospital mortality after major amputation of the lower limbs for critical ischemia. Open Atheroscler Thromb J. 2009; 2:4-5.
14. Ogeng'O JA, Obimbo MM, King'ori J, Njogu SW. Pattern of limb amputation among rural Kenyan children and adolescents. J Prosthetics Orthotics. 2010; 22(3):157-61. DOI: 10.1097/JPO.0b013e3181e94834
15. Akinyoola AL, Oginni LM, Adegbehingbe OO, Orimolade EA, Ogundele OJ. Causes of limb amputations in Nigerian children. West Afr J Med. 2006; 25(4):273-5. PMID: 17402514
16. Bickler SW, Sanno-Duanda B. Bone setter's gangrene. J Pediatr Surg. 2000; 35(10):1431-3. PMID: 11051143 DOI: 10.1053/jpsu.2000.16406
17. Garba ES, Deshi PJ. Traditional bone setting: a risk factor in limb amputation. East Afr Med J. 1998; 75(9):553-5. PMID: 10493061
18. Nwankwo OE, Katchy AU. Limb gangrene following treatment of limb injury by traditional bone setter (Tbs): a report of 15 consecutive cases. Niger Postgrad Med J. 2005; 12(1):57-60. PMID: 15827600
19. Nwachukwu BU, Okwesili IC, Harris MB, Katz JN. Traditional bonesetters and contemporary orthopaedic fracture care in a developing nation: historical aspects, contemporary status and future directions. Open Orthop. 2011; 5(1):20-6. PMID: 21270953 DOI: 10.2174/1874325001105010020
20. Stewart BT, Gyedu A, Tansley G, Yeboah D, Amponsah-Manu F, Mock C, et al. Orthopaedic trauma care capacity assessment and strategic planning in Ghana: mapping a way forward. J Bone Joint Surg Am. 2016; 98(23):e104. PMID: 27926686 DOI: 10.2106/JBJS.15.01299
Received: 2019/10/1 | Accepted: 2020/01/11 | Published: 2020/02/17 | ePublished: 2020/02/17
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Attribution-NoneCommercial CC BY-NC
