


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jsurgery.bums.ac.ir/article-1-181-en.html




Effects of ketorolac versus pethidine on the management of postoperative acute pain and complications after hemorrhoidectomy
Mohammad Reza Ghasemian Moghaddam1![]() , Mahmoud Ganjifard2
, Mahmoud Ganjifard2![]() , Saeedeh Ghasemi3*
, Saeedeh Ghasemi3*![]()
1Assistant Professor of Surgery, School of Medicine, Cardiovascular Diseases Research Center, Birjand University of Medical Sciences, Birjand, Iran
2Assistant Professor, Department of Anesthesia, Birjand University of Medical Sciences, Birjand, Iran
3Student Research Committee, Birjand University of Medical Sciences, Birjand, Iran
Received: March 05, 2019 Revised: September 01, 2019 Accepted: September 01, 2019
|
Abstract Introduction: Pain management is one of the most essential components of postoperative care. Nowadays, the common treatment methods for pain include the use of two large groups of analgesics, namely opioids and nonsteroidal anti-inflammatory drugs (NSAIDs). Therefore, the present study aimed to compare the effects of ketorolac (i.e., a non-inflammatory drug) and pethidine (i.e., a synthetic opioid pain medication) on pain and complications due to hemorrhoidectomy. Methods: This randomized controlled trial included 90 patients with hemorrhoids who underwent hemorrhoidectomy at Imam Reza Hospital in Birjand, Iran, from May 2017 to 2018. The participants were assigned into two groups, namely ketorolac group who received ketorolac therapy and pethidine group who received pethidine. The severity of pain and complications were measured immediately, as well as at 6, and 12 hours after surgery in both study groups. The quantitative data were expressed as mean and percentage. Data analysis was performed using SPSS software (version 22.0) through Mann-Whitney, Friedman, and Chi-square tests. A p-value less than 0.05 was considered statistically significant. Results: According to the obtained results, out of 90 patients with hemorrhoid, 70.3% were males. The mean age of the participants was 48.29±8.8 years, and there was no significant difference between two study groups regarding age (47.2±8.7 years in the pethidine group, and 49.4±9 years in the ketorolac group, P=0.196). In the ketorolac group, the mean pain scores were 2.33±1.36, 2.28±1.00, and 1.57±0.75, immediately, as well as at 6, and 12 hours after surgery, respectively. In addition, in the pethidine group, the mean pain scores were obtained at 3.15±1.61, 2.64±1.00, and 1.97±0.69, immediately as well as at 6, and 12 hours after surgery, respectively. Accordingly, the pain level was significantly lower in ketorolac group, compared to that in the pethidine group (P<0.05). However, the pain level was higher at 24 hours after surgery in ketorolac group than that in the pethidine group; nevertheless, the difference was not statistically significant (P=0.996). Conclusions: The findings of the present study suggest more significant therapeutic effects of nonsteroidal NSAIDs, compared to opioid drugs on pain after hemorrhoidectomy. Key words: Hemorrhoidectomy, Ketorolac, Meperidine, Pain management |
Introduction
Hemorrhoids are common anorectal conditions and are defined as the symptomatic enlargement and distal displacement of normal anal cushions (1). Hemorrhoids affect about 5% of the general population, and particularly more than 50% of people over the age of 50 displayed symptoms of hemorrhoids (2). The most common symptom of hemorrhoids is painless rectal bleeding with a bowel movement, which is described by patients as the release of droplets into the toilet bowl. The blood is typically red as hemorrhoidal tissue has direct arteriovenous communication (3). The treatment of hemorrhoids varying from correct dietary to radical operation relies on the severity
of symptoms (4, 5). Typical open or closed hemorrhoidectomy is one of the most common surgical treatments for hemorrhoids (6).
Anal surgery is commonly performed as a non-ambulatory operation due to concerns about the lack of management of postoperative pain and surgery-related problems (7, 8). This surgery, the same as other treatment methods, includes complications, such as bleeding, urinary retention, infection, fecal impaction and compression, internal anal sphincter damage, and pain (9). Pain can lead to severe discomfort and delay return to normal daily activities (10). Pain management after the operation is of great importance in order to make hemorrhoidectomy more tolerable for the patient. The postoperative pain level depends on several factors, including patient's tolerance, anesthetic procedure, surgical approach, and postoperative pain killers (11).
A wide range of drugs and treatment methods are used to reduce post hemorrhoidectomy pain, including calcium channel blockers, glyceryl trinitrate, botulinum toxin, ketorolac, metroni-dazole, gabapentin, morphine, cholestyramine, sucralfate, transcutaneous electrical nerve stimulation (12), and ischiorectal fossa block (13). According to the results of this study, a mixture of oral and topical injection of ketorolac displayed more significant effects on postoperative pain management than narcotic therapy, after excisional hemorrhoidectomy (12). Opioids have many side effects, including nausea, vomiting, ventilating depression (14), and urinary retention (1). However, NSAIDs do not exhibit these complications; therefore, these two types of treatments can be compared during the management of postoperative pain (14). Postoperative prevention and treatment are among the main issues in postoperative care which plays an important role in the pain management and improvement of the general condition of patients. Therefore, the present study aimed to examine and compare the effects of ketorolac (i.e., a non-inflammatory drug) and pethidine (i.e., a synthetic opioid pain medication) on postoperative pain and complication management after hemorrhoidectomy.
Methods
This randomized controlled clinical trial was conducted on 90 patients with hemorrhoid who underwent hemorrhoidectomy at Imam Reza Hospital in Birjand, Iran, from May 2017 to 2018. The study protocol was approved by the Ethics Committee of Birjand University of Medical Sciences (Ir.bums.REC.1397.48). Moreover, this study was registered on the Iranian clinical trial site (IRCT20140519017756N44). The informed consent was obtained from all participants or their close relatives, and all of them were fully informed of the research procedure and objectives.
The sample size was initially estimated at 43 in each group with α= 0.05 and a power of 80%. Regarding the sample attrition, the sample size was eventually obtained at 45 in each group; moreover, the effect size in this study was calculated at 0.6.
The inclusion criteria were: 1) >18 years of age, 2) type 1 and 2 patients according to the latest version of the American Society of Anesthesiologists physical status classification system, and 3) lack of the utilization of opioid relievers or pain killers in large scale. On the other hand, the patients with a history of pulmonary diseases, asthma, peptic ulcer, abdominal surgery, and allergy to NSAIDs, as well as those with liver and renal diseases,
drug addiction, bronchial asthma, gestational hypertension, preeclampsia, coagulation disorder, long length of operation (>20 min), bleeding, and postoperative complications were excluded from the study. All patients who were included in this study were trained to use a Visual Analogue Scale (VAS) a few hours prior to the operation. Those who met the inclusion criteria were divided into two groups, namely pethidine group who received pethidine, and ketorolac group who received ketorolac using simple randomization and random number table.
Moreover, the anesthesia was induced using intravenous midazolam 1mg/kg followed by fentanyl 2 mg/kg and propofol 2mg/kg. The operation was performed utilizing a specific protocol by a surgeon. Immediately after the operation, the first group received 0.5 mg/kg of intravenous pethidine followed by 50 mg/kg of pethidine three times a day in an injection, and the second group received a mixture of intravenous ketorolac 0.9 mg/kg with ketorolac TDS 30 mg/kg.
Each patient was trained by an experienced technician who was blinded to the patient's prescription to rate their pain severity using VAS. Moreover, all patients were investigated and examined after transferring to the recovery phase with full consciousness at zero (when the patient wakes up and understands the environment at the beginning of recovery), 6, 12, and 24 hours after entering the recovery.
It should be noted that if the VAS was more than 3cm for 2 times with an interval of 15 minutes, then an additional pethidine 0.5 mg/kg was injected to the patient since no patient should not suffer from pain in any group. Finally, the results of each patient review were recorded in a checklist.
Other information about the patients, including demographic characteristics and drug side effects, were collected in a standard checklist based on the research objectives. In all patients, the severity of post hemorrhoidectomy pain was evaluated using VAS. This pain measurement scale is a 10-cm ruler ranging from 0-10 indicating no and extreme pains, respectively. Moreover, the scores less than 3, between 3 and 7, and greater than 7 cm represents mild, average, and severe pain.
The data analysis was performed using SPSS software (version 22.0). The quantitative results were expressed as mean (±SD) and percentage (frequency). The Mann-Whitney U and Chi-square tests were used after confirming the normal distribution of the quantitative variables. A p-value less than 0.05 was considered statistically significant.
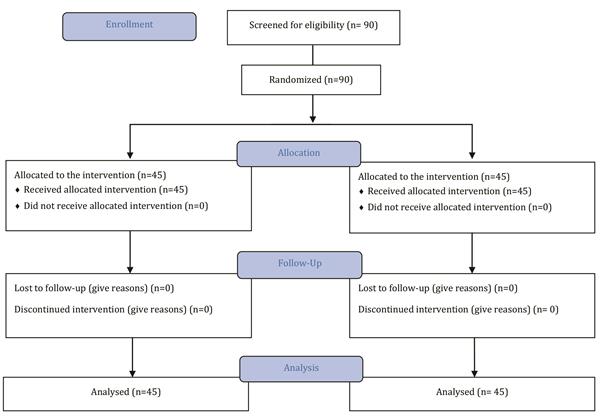
Figure 1: Sampling method flowchart
Results
The mean age of the participants was 48.29±8.8 years, and the mean ages of the participants in pethidine and ketorolac groups were 47.2±8.7 and 49.4±9 years, respectively. Moreover, no significant difference was observed between the two groups regarding age (P=0.196). The majority of patients in pethidine (73.3%) and ketorolac groups (66.7%) were male, which was not statistically significant (P=0.490, Table 1).
According to the Shapiro test, P was lower than 0.05 in two groups at different times indicating the non-normal distribution of the data. Therefore, the Mann-Whitney U test showed that mean pain
level was significantly lower in ketorolac group, compared to that in the pethidine group, immediately (2.33±1.36, 3.15±1.61, P=0.013), as well as at 6 (2.28±1.00, 2.64±1.00, P=0.040), and 12 hours after hemorrhoidectomy (1.57±0.75, 1.97±0.69, P=0.009). However, the mean pain level was revealed to be higher in ketorolac group (1.37±0.71), compared to pethidine group (1.28±0.45) at 24 hours after hemorrhoidectomy; however, the difference was not statistically significant (P=0.996, Table 2).
The results of the Friedman test showed that the mean pain immediately, as well as at 6, 12, and 24 hours after hemorrhoidectomy had significantly decreasing trend in both pethidine and ketorolac group (P=0.001, Table 3). As it is shown in Table 4, pethidine decreases the pain significantly more than ketorolac at 12 and 24 hours after hemorrhoidectomy (P=0.02). However, this decreasing trend was observed at other times.
The evaluation of pain severity reported by the
|
Table 1: Comparison of gender distribution in two study groups |
||||
|
Group |
||||
|
Gender |
Pethidine N (%) |
Ketorolac N (%) |
Chi-square |
P-value |
|
Male Female |
33(73.3) 12(26.1) |
30(37.66) 15(33.3) |
0.476 |
P=0.490 |
|
Table 2: Comparison of mean pain level at various times after hemorrhoidectomy |
||||
|
Item |
Ketorolac (Mean± SD) |
Pethidine (Mean± SD) |
Z-value |
P-value |
|
Immediately |
2.33±1.36 |
3.15±1.61 |
-2.49 |
0.013* |
|
6 hours |
2.28±1.00 |
2.64±1.00 |
-2.05 |
0.040* |
|
12 hours |
1.57±0.75 |
1.97±0.69 |
-2.60 |
0.009* |
|
24 hours |
1.37±0.71 |
1.28±0.45 |
-0.005 |
0.996 |
|
Shapiro-Wilk test had p-value lower than 0.05 in all categories * Significant difference between ketorolac and pethidine groups |
||||
|
Table 3: Comparison of mean pain variations at various times after hemorrhoidectomy |
||
|
Time |
Ketorolac (Mean Rank) |
Pethidine (Mean Rank) |
|
Immediately |
2.78 |
3.16 |
|
6 hours |
3.17 |
3.04 |
|
12 hours |
2.23 |
2.26 |
|
24 hours |
1.82 |
1.53 |
|
Chi square (P-value) |
36.83 (0.001*) |
59.29 (0.001*) |
|
* There is a significant trend |
||
|
Table 4: Comparison of mean pain variations at various times after hemorrhoidectomy |
|||
|
Time |
Ketorolac (Mean± SD) |
Pethidine (Mean± SD) |
P-value |
|
Pain level changes in 0,6 hours |
0.04±1.5 |
0.5±1.6 |
P=0.166 |
|
Pain level changes in 6,12 hours |
0.7±1.1 |
0.7±0.8 |
P=0.788 |
|
Pain level changes in 12,24 hours |
0.2±1.03 |
0.67±0.7 |
P=0.02* |
|
Shapiro-Wilk had p-value lower than 0.05 in all categories * Different decreasing trends between ketorolac and pethidine groups |
|||
participants suggests a significant difference between ketorolac and pethidine groups regarding the pain at 6 and 24 hours after the operation (P<0.05, Table 5). Accordingly, the majority of participants in ketorolac group experienced mild pain at 6 hours after surgery and all patients in the pethidine group had mild pain after 24 hours. However, no significant difference was observed between the two groups in terms of the pain level at 0 and 12 hours after operation (P>0.05). Furthermore, the results of the present study revealed that all patients in both ketorolac
and pethidine groups displayed no specific complications after hemorrhoidectomy.
Discussion
Pain normally occurs at different degrees and
|
Table 5: Comparison of pain intensity at 0, 6, 12 and 24 hours after hemorrhoidectomy in study groups |
||||||
|
Study groups |
|
|||||
|
P-value |
Chi-square |
Ketorolac N(%) |
Pethidine N(%) |
|
Pain intensity |
|
|
0.528 |
0.566 |
27(60) |
24(52.2) |
Mild |
Immediately |
|
|
18(40) |
22(47.8) |
Moderate |
||||
|
0.02* |
5.926 |
31(68.9) |
20(43.5) |
Mild |
6 hours |
|
|
14(31.1) |
26(56.5) |
Moderate |
||||
|
0.592 |
0.573 |
38(84.4) |
36(78.3) |
Mild |
12 hours |
|
|
7(15.6) |
10(21.7) |
Moderate |
||||
|
0.012* |
6.566 |
39(86.7) |
45(100) |
Mild |
24 hours |
|
|
6(13.3) |
0(0) |
Moderate |
||||
|
* Significant association between ketorolac and pethidine groups regarding pain intensity |
||||||
inevitability after all surgical procedures which is accompanied by adverse physiological effects. The postoperative pain level depends on many factors, including patient's tolerance, anesthetic procedure, surgical approach, and the utilization of postoperative pain killers (11). According to the findings of this study, there was a significant difference between pethidine and ketorolac groups in terms of mean pain intensity in different hours. Accordingly, the mean pain intensity score was significantly lower in the ketorolac group than that in the pethidine group immediately, as well as at 6, and 12 hours after the operation. However, the pain level was higher at 24 hours after the operation in the ketorolac group than that in the pethidine group; nevertheless, the difference was not significant. The results also showed a significant difference between the groups receiving pethidine and ketorolac regarding the mean pain intensity immediately, as well as at 6, 12, and 24 hours after hemorrhoidectomy (P=0.001).
According to the literature, in addition to pain management effects, ketorolac reduces the need for opioids use (15, 16). In the same line, Timothy et al. stated that the frequency of opioid drug use was significantly lower in patients receiving ketorolac than those treated with meperidine (17). Furthermore, Imani et al. examined the effects of adding dexmedetomidine to paracetamol or ketorolac on post-cesarean pain and related complications. They revealed that the patients receiving a mixture of dexmedetomidine and ketorolac experienced lower levels of pain significantly, compared to those who received a mixture of dexmedetomidine and paracetamol (18).
Another study compared the effect of a single use of paracetamol with a mixture of tramadol
and ketorolac in post hemorrhoidectomy pain management. The results of the aforementioned study showed that the continuous infusion of a mixture of tramadol and ketorolac improved pain management and reduced the length of hospital stay (10). On the other hand, Sun Yeul Lee et al. investigated the effect of a mixture of paracetamol and ketorolac as well as a mixture of morphine with paracetamol on post-thyroidectomy pain management. They observed no difference between the effects of ketorolac and paracetamol on postoperative pain (19). These results were supported by a study conducted by Elena Neri et al. who investigated the effect of a mixture of ketorolac with tramadol on acute pain due to fracture or dislocation among children. However, they reported a lower level of related side effects, such as vomiting in those receiving ketorolac (20).
The results of this study showed a significant difference between pethidine and ketorolac groups regarding the pain intensity at 6 and 24 hours after the operation, whereas there was no significant difference between the two groups in terms of pain intensity immediately, as well as at 12 hours after the operation. Gin et al. measured the mean pain intensity by VAS in two groups of patients receiving pethidine and ketorolac after cesarean surgery. They found that ketorolac was also more effective in reducing postoperative pain, compared to pethidine(21).
Similarly, Forrest et al. revealed that the pain-relieving effect of ketorolac was more significant than other opioid drugs among children who underwent tonsil surgery (22). Shankariah et al. reported that the mean post-cesarean pain intensity was significantly lower in subjects who received ketorolac as an NSAID and tramadol as an opioid, compared to patients who received placebo. In addition, a more significant difference was observed between subjects who consumed tramadol and those who consumed ketorolac (23).
These results were inconsistent with the findings obtained from this study, which may be due to differences in surgical procedure and type of administered opioid drug for pain management. Given that cyclooxygenase-2 plays a magnificent role in the central and peripheral mechanism of pain in trauma or injuries, an ideal drug for the treatment of acute inflammatory pain is the one that targets and inhibits cyclooxygenase-2 in both the peripheral and central regions (24). Therefore, more significant reducing effects of ketorolac on pain, compared to pethidine are due to the anti-inflammatory properties of ketorolac.
In addition, the participants in the current study reported no specific complications after hemorrhoidectomy, whereas a study conducted by Gin et al. showed adverse effects, such as dizziness and vomiting in patients who received pethidine (21). In general, the findings of this study
showed significant effects of NSAIDs on post hemorrhoidectomy pain than those of opioids. Due to the unknown coagulation disorders and lack of clear and complete medical history of bleeding disorders as well as limited sample size, further research is recommended to investigate the side effects of NSAIDs and their therapeutic effects on postoperative pain after any type of surgical procedures.
Conclusions
The therapeutic effect of NSAIDs was shown to be more significantly effective than that of other opioid drugs on pain and complications after hemorrhoidectomy.
Acknowledgments
The authors would like to thank Birjand University of Medical Sciences, Birjand, Iran, and the center for Development of Clinical Research of Razi and Imam Reza Hospital for their consultation, editorial, and statistical assistance (Grant number: 455418 ).
Funding
This study was funded by Birjand University of Medical Sciences, Birjand, Iran.
Conflict of Interest
There is no conflict of interests to be declared.
References
1. Lohsiriwat V. Hemorrhoids: from basic pathophy-siology to clinical management. World journal of gastroenterology: WJG. 2012;18(17):2009.
2. Basdanis G, Papadopoulos V, Michalopoulos A, Apostolidis S, Harlaftis N. Randomized clinical trial of stapled hemorrhoidectomy vs open with Ligasure for prolapsed piles. Surgical Endoscopy And Other Interventional Techniques. 2005;19(2):235-9.
3. Aigner F, Gruber H, Conrad F, Eder J, Wedel T, Zelger B, et al. Revised morphology and hemodynamics of the anorectal vascular plexus: impact on the course of hemorrhoidal disease. International journal of colorectal disease. 2009;24(1):105-13.
4. Acheson AG, Scholefield JH. Management of haemorrhoids. Bmj. 2008;336(7640):380-3.
5. Kaidar-Person O, Person B, Wexner SD. Hemorrhoidal disease: a comprehensive review. Journal of the American College of Surgeons. 2007;204(1):102-17.
6. Ortiz H, Marzo J, Armendariz P. Randomized clinical trial of stapled haemorrhoidopexy versus conventional diathermy haemorrhoidectomy. British journal of surgery. 2002;89(11):1376-81.
7. Palazzo F, Francis D, Clifton M. Randomized clinical trial of Ligasure™ versus open haemorrhoidectomy. British Journal of Surgery. 2002;89(2):154-7.
8. Rahimi M, Makarem J, Maktobi M. Post hemorrhoidectomy pain control: rectal Diclofenac versus Acetaminophen. Tehran University Medical Journal. 2009;67(1).
9. Billiar T, Andersen D, Hunter J, Brunicardi F, Dunn D, Pollock RE. Schwartz's principles of surgery: McGraw-Hill Professional; 2004.
10. Marino F, Novelli E, Manca G. Efficacy of Paracetamol Versus Tramadol Plus Ketorolac for Pain Control after Hemorrhoidectomy: A Prospective Randomized Trial. Gastroenterol Hepatol Open Access. 2016;
4(6):00122.
11. Joshi G, Neugebauer E. Evidence‐based management of pain after haemorrhoidectomy surgery. British Journal of Surgery. 2010;97(8):1155-68.
12. Emile SH. Evidence-based review of methods used to reduce pain after excisional hemorrhoidectomy. Journal of Coloproctology (Rio de Janeiro). 2019;
39(1):81-9.
13. Nadri S, Mahmoudvand H, Rokrok S, Tarrahi MJ. Comparison of two methods: Spinal anesthesia and ischiorectal block on post hemorrhoidectomy pain and hospital stay: A randomized control trial. Journal of Investigative Surgery. 2018;31(5):420-4.
14. Merrikhihaghi S, Farshchi A, Farshchi B, Farshchi S, Abedin-Dorkoosh F. Tramadol versus diclofenac in pain management after cesarean section: A cost analysis study. Journal of Pharmacoeconomics and Pharmaceutical Management. 2015;1(1/2):22-4.
15. Carney DE, Nicolette LA, Ratner MH, Minerd A, Baesl TJ. Ketorolac reduces postoperative narcotic requirements. Journal of pediatric surgery. 2001;
36(1):76-9.
16. De Oliveira GS, Agarwal D, Benzon HT. Perioperative single dose ketorolac to prevent postoperative pain: a meta-analysis of randomized trials. Anesthesia & Analgesia. 2012;114(2):424-33.
17. Pavy TJ, Paech MJ, Evans SF. The effect of intravenous ketorolac on opioid requirement and pain after cesarean delivery. Anesthesia & Analgesia. 2001;
92(4):1010-4.
18. Imani F, Rahimzadeh P, Faiz H-R, Nowruzina S, Shakeri A, Ghahremani M. Comparison of the post-caesarean analgesic effect of adding dexmedeto-midine to paracetamol and ketorolac: A randomized clinical trial. Anesthesiology and pain medicine. 2018;8(5).
19. Lee SY, Lee WH, Lee EH, Han KC, Ko YK. The effects of paracetamol, ketorolac, and paracetamol plus morphine on pain control after thyroidectomy. The Korean journal of pain. 2010;23(2):124.
20. Neri E, Maestro A, Minen F, Montico M, Ronfani L, Zanon D, et al. Sublingual ketorolac versus sublingual tramadol for moderate to severe post-traumatic bone pain in children: a double-blind, randomised, controlled trial. Archives of disease in childhood. 2013;98(9):721-4.
21. Gin T, Kan A, Lam K, O'Meara M. Analgesia after caesarean section with intramuscular ketorolac
or pethidine. Anaesthesia and intensive care. 1993;21(4):420-3.
22. Forrest JB, Heitlinger EL, Revell S. Ketorolac for postoperative pain management in children. Drug safety. 1997;16(5):309-29.
23. Shankariah M, Mishra M, Kamath RA. Tramadol versus ketorolac in the treatment of postoperative pain following maxillofacial surgery. Journal of maxillofacial and oral surgery. 2012;11(3):264-70.
24. Wong JO-N, Tan TD-M, Cheu N-W, Wang Y-R, Liao C-H, Chuang F-H, et al. Comparison of the efficacy of parecoxib versus ketorolac combined with morphine on patient-controlled analgesia for post-cesarean delivery pain management. Acta Anaesthesiologica Taiwanica. 2010;48(4):174-7.
Received: 2019/03/5 | Accepted: 2019/09/1 | Published: 2019/09/22
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Attribution-NoneCommercial CC BY-NC
